A rough, and incomplete catalogue of Transgender conversion efforts in the Anglo American psychiatric complex
This piece is written in the main a short index to the history of trans medical conversion efforts in the 20th century English speaking world. Before getting into this, I have a couple of cautionary notes for readers that I think need to go first. One is about the racism that was core to so much of sexology and yet seems to very easily go missing. Another is about the fact when we are looking at history through the eyes of people who tortured trans folks, we need to be careful not to inherit what they say as “the truth”, even if we believe they might have been reporting their evidence faithfully.
The white supremacist origins of understanding transness as a “perversion”.
As a starting point here, as absolutely critical context to understanding the evolution of conversion efforts in “The West”, the origins of sexology and the study of transgender behaviours were profoundly colonial and racist and absolutely tied up in the history of the eugenic theory of “scientific racism”, now returning to popularity among white supremacist scientists as “race realism”. An example of this is in C.G. Seligman’s paper Sexual Inversion Among Primitive Races (1902) which distinguishes between subjects expressing “psychical resemblances to the opposite sex” (borrowing Albert Moll’s concept of “psychosexual hermaphroditism”, one of the earlier forms of the “female brain trapped in a man’s body” concept) and same sex sexual activity (“sodomy”) and emphasising that much research had previously focused mainly on “grosser forms of perversion” (trans-gender identity) overlooking homosexual practices with examples such as cultures where it was common for men to use transfeminine sex workers with the stigma mainly lying on the sex workers rather than their johns. Seligman’s “novel” discovery is that counter to existing beliefs that transgender and homosexual behaviours being a form of degeneracy formed by decadent cultural advancement, it is instead widespread practice and acceptance of same sex sexuality and gender-crossing activities were prolific through many cultures he refers to as “savages”.
It seems obvious, but needs stating clearly here, that the only two possibilities he considers here are either on the one hand what he calls “perversion” resulting from cultural degeneration of decadent “oriental luxury or advanced civilization”, or on the other hand it being more a phenomenon of “primitive races”. The conceivable possibilities available to Seligman here are constrained by the racist ideology he is operating within. It is one profoundly white supremacist model or another. This is an object example of this white supremacist ideology baked into the heart of sexological attempts to understand LGBTQ experiences and expressions/behaviours as something which must be purified or corrected against, but it is far from the only one, and I include it here as a means of hopefully inserting a strong reminder that the science of sexual psychology is not a neutral evidence driven practice but an ideological one, and has been from the very beginning.
As I’ll show going through this (incomplete, but nevertheless quite long) list of papers I’ve found on the topic, we’ll see that even as psychosexual therapists over time discover that they are unable to “cure” cross-sex identity, they retain this principle that it is something which is pathological, regrettable, and this continues right up until the present for many psychoanalytic therapists on the gender identity grift. The original resistance to conversion therapy was not (as you might if you were less committed to ideologically white supremacist and coercive psychiatric structures) about whether sexual orientation and gender identity change efforts were a form of violence against the person, but about the fact that they simply didn’t work in practice. The lack of significant accountability for these long running roots has led generally to a failure to abolish the racist eugenic puritanism at the core of sexology and its concerns around degeneracy. It’s far to easily (and frequently) dismissed as an aberration which maybe threw off some of the method without understanding it as a driving rationale for constructing the medical techniques being produced by it and the implicit goals and values that are baked into these approaches.
A warning before we delve into the cis gaze
Overall, looking through history in the form of scientific research papers, as with the previous warning, we risk ourselves adopting aspects of the perspective of people who professionally tortured or neglected trans people for many decades. Even a critical view of these practices as they were self-reported by the practitioners can not give us a fully fledged insight into the experience of trans people facing conversion efforts in a medical setting. I had the good fortune to be provided with a copy of the proceedings of the 1974 First National Transvestite/Transsexual Conference in Leeds, United Kingdom, which I transcribed a while ago. Views shared by transsexual and transvestite people of the English psychiatric system’s handling of transsexual needs were summarised in the conference notes rather dimly:
The Maudsley Hospital [a psychiatric institution in the UK]
One member of the group had recently undergone an unsuccessful course of aversion therapy there. She felt with the rest of us who had not had that privilege (?), that there was no place for such therapy in the resolution of our problem. Dr. Goldberg who had been in charge of this therapy has moved his shocking habits down to Oxford, leaving the field open for Dr. Isaac Marks.
Psychiatrists:
Limited in their individual experience. An adjustment rather than a curative approach must be concentrated on. The Maudsley type of experience in using aversion therapy was only valid if, by using it in a strictly controlled way, they could authoritatively discredit it for ever.
Trans women who had undergone torture for being trans were clear many decades ago that coercive conversion efforts had no purpose. This is one of a few such pieces of nearly direct evidence around, and it’s still very much a fleeting and inadequate portrait of the suffering imposed on trans people. Dr Marks (and colleagues) are among the catalogue of research papers here.
I’m always interested in others if people know of them and want to reach out to me on Twitter.
1949: The Western adoption of the word Transsexual
The original importer of the term “Transsexual” into the English speaking scientific sphere was David Oliver Cauldwell in his essay Psychopathia Transsexualis for Sexology Magazine. This point in history is important, because it is the point at which sexologists and clinicians first have a terminology for distinguishing gender identity variations from variations in sexuality, and this enables the innovation of starting to build a specific idea of attempting to cure each separately (although this would take some years to actually disambiguate the two).
The same quasi-eugenicist framing from early sexology is still very much a feature of how sexologists thought of transness. This belief system lies at the root of thinking of trans identity as an illness at all. Cauldwell opens:
Among both sexes are individuals who wish to be members of the sex to which they do not properly belong. Their condition usually arises from a poor hereditary background and a highly unfavourable childhood environment. Proportionately there are more individuals in this category among the well-to-do than among the poor. Poverty and its attendant necessities serve, to an extent, as deterrents.
When an individual fails to mature according to his (or her) proper biological and sexological status, such an individual is psychologically (mentally) deficient. The psychological condition is in reality the disease.
So above we have “poor hereditary background” — the idea that transness is a condition of weak genes somehow, and then transness as a disease or mental deficiency. The article goes on to describe the life history and transition pathway undertaken by ‘Earl’, a transmasculine person registered female at birth. Cauldwell goes on to describe Earl as narcissistic, lacking in the masculine characteristics Earl liked to see himself. Cauldwell describes Earl having asked for genital reassignment surgery (knowing that this practice happened sometimes to intersex people) which Cauldwell asserts is mistaken because he examined Earl and found his genitals to be “the perfect feminine formation”. Cauldwell describes how sometimes intersex people are transsexed, or “after accidents” (uncited).
The 1950s
We start here very early with an example of a problem we will see quite a lot in the field — scientific positivism has a bias towards not reporting negative results directly. Instead we can easily find a great many papers where the authors candidly discuss that all efforts they are aware of to cure “transsexualism” have failed. We don’t always find clear documentation of the nature of those efforts, because almost no one was publishing failed experiments. Transgender therapies have been an open season test bed for practitioners. The perceived harms of affirming the trans person’s identity were considered justification enough to permit other rather more direct harms in the aim of building a cure and then just rarely document how they failed. The harms that were done are difficult to find in the scientific literature, despite regular reference to their failure.
As the truism goes, it’s hard-to-impossible to prove a negative, that no such “curative” technique exists (with the begged question here being whether transness is a pathology to be cured in the first place). The search for such a technique, if it doesn’t exist, may rationalise a literally infinite amount of experimentation and suffering imposed upon unwilling transgender patients who just want to be prescribed HRT and/or surgery and enabled to get on with life. People evaluating moral arguments around the idea of conversion efforts must very seriously take into account the relatively large body of existing evidence across clinical research that such efforts were being undertaken already for a long time and proved fruitless.
We must take into account the already undertaken harm against trans people, the wide scale violation of trans people’s human dignity and personal autonomy and agency, and take seriously the moral duty of clinicians not to use their position of power to impose their views of what’s best over the well-being of trans patients. So our first English language comment on the topic of efforts to reconcile trans people’s identities with our anatomies comes from Harry Benjamin (who had previously met and at the very least corresponded with Magnus Hirschfeld of the Institute for Sexual Research in Berlin before the Nazis destroyed it, and so knew more than most about the history of research before research clearly and unambiguously conscious of the existence of trans people had reached America).
“All therapy , in cases of transsexualism — to the best of my knowledge — has proved useless as far as any cure is concerned. I know of no case where even intensive and prolonged psychoanalysis had any success. If we are dealing with a constitutional deviation, we can hardly expect to influence it .”…”In my opinion, psychotherapy for the purpose of curing the condition is a waste of time . A basic conflict would be too firmly anchored in the constitution. All that the psychiatrist can possibly do is to relax tension, to develop and reinforce realistic thinking , and to supply guidance. That, of course, is not a cure.” — Benjamin, H. (1954). Transsexualism and Transvestism — A Symposium. American Journal of Psychotherapy, 8(2), 219–230. doi:10.1176/appi.psychotherapy.1954.8.2.219. https://sci-hub.se/10.1176/appi.psychotherapy.1954.8.2.219
“With the significant exception of the psychosexual deviants, maleness (as defined by the culture) and male body structure and femaleness (so defined) and female body structure are so universally associated one with another that the characteristic personality type has been assumed to be a simple consequence of the structural and biochemical specificities of each sex. Yet a nagging doubt has always existed because of the notable exception of the invert.”
— Eisenberg, L. (1957). Progress in neuropsychiatry. The Journal of Pediatrics, 51(3), 334–349. doi:10.1016/s0022–3476(57)80210–8 https://sci-hub.se/10.1016/S0022-3476(57)80210-8
“SEX DIFFERENCES IN INVERSION One interesting question related to the present discussion is whether or not the incidence of inversion differs in males and females. Mowrer, in a personal communication to the writer, raised this question in connection with a study of sex-role preference patterns in children ~ which, among other things, provides information on differences in the acceptance of sex roles and on preferences for the role of the opposite sex in boys compared to girls. ”
— Brown, D. G. (1957). The development of sex-role inversion and homosexuality. The Journal of Pediatrics, 50(5), 613–619. doi:10.1016/s0022–3476(57)80228–5 — sci-hub.se/10.1016/S0022–3476(57)80228–5
“The essential basis of inversion (i.e., the process in which an individual adopts the psychological identity typical of the opposite sex) appears to be an early, continuing, emotionally deep-rooted identification with, as well as preference for, the sex-role of the opposite sex. Expressed preference per se for the role of the opposite sex may or may not be based on identification with that role (2). Thus, for example, if a girl’s basic and underlying identification is with the feminine role, the fact that she may show a preference for the masculine role during childhood does not necessarily indicate sex-role inversion. It is quite likely that many girls prefer much that is associated with the masculine role without having formed a fundamental identification with that role”
— Brown, D. G. (1957). Masculinity-femininity development in children. Journal of Consulting Psychology, 21(3), 197–202. doi:10.1037/h0044827. sci-hub.se/10.1037/h0044827
“The origin and earliest occurrence of sex-role preference is a problem that awaits research investigation. That definite preferences exist in young children for one or the other sex role, however, has been reasonably well demonstrated by several studies.” Brown, D. G. (1958).
— Sex-role development in a changing culture. Psychological Bulletin, 55(4), 232–242. doi:10.1037/h0039862 — sci-hub.se/10.1037/h0039862
“Homosexuality refers to sexual activity or desire for such activity between two members of the same sex, whereas sexual inversion refers to identification with and adoption of the psychological identity of the opposite sex.”, references to childhood experiences of trans-sex identification, as well as distinguishing transvestism from trans-sex identification.
— Brown, D. G. (1958). Inversion and homosexuality. American Journal of Orthopsychiatry, 28(2), 424–429. doi:10.1111/j.1939–0025.1958.tb03761.x — sci-hub.se/10.1111/j.1939–0025.1958.tb03761.x
“These considerations may be important in evaluating prognosis in psychotherapy. If, as has never been reported in any case, psychotherapy were to return him to an heterosexual outlook, he would have to give up his equivocal eminence and presumably assume some role in the social structure — which could hardly help being fairly low, inasmuch as he is a poorly educated foreigner.”
— Article on a transsexual who refused psychotherapy and demanded transition surgery. — NORTHRUP, G. (1959). Transsexualism. A.M.A. Archives of General Psychiatry, 1(3), 332. doi:10.1001/archpsyc.1959.03590030116013
1960s
“Treatment and Prevention. So far as is known there is not a single case of clearly established adult inversion on record in which the person’s inverted role has been replaced with a normal sex role by means of psychotherapy or, for that matter, by any other means. While this does not necessarily mean that a restructuring of personality is impossible, especially given a strong desire on the part of the patient to effect such a change, it does mean that an inverted individual is likely to remain so throughout his life”.
— Brown, D. G. (1960). Psychosexual Disturbances: Transvestism and Sex-Role Inversion. Marriage and Family Living, 22(3), 218. doi:10.2307/347641 — https://sci-hub.se/10.2307/347641
1970s
Below we have one of the rare follow up studies of the sorts of aversion therapy which were happening in the UK in the late 1960s and in this case published in 1970 (carried out by among others, the clinician Marks who was called out as being particularly brutal in the earlier reference to UK trans people’s own perspectives on conversion therapies). This study covered a grab bag of 24 research subjects who were subjected to aversion therapy, either transsexuals, transvestites or people with fetishes (e.g. for rubber or shoes), and sadomasochists.
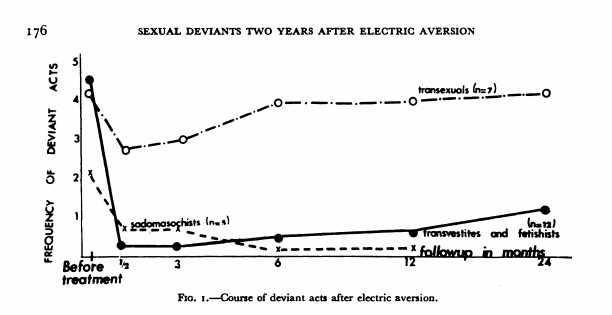
The results are fairly disastrous, but aversion therapy continued in various forms for many years all the same. As is visible in the graph, transsexuals experienced a limited response to the conversion therapy in any case, and a return to transsexuality. I should point out here, that this may not be a result of the specific difficulty in curing transsexuality as such —some similar studies of the era found rates as high as 50% of supposedly curing homosexual desires and fantasies. What is specific to transsexuality here is the fact that it is acutely difficult to just lie about being transsexual to the psychologists you interact with, in ways where homosexuals and transvestites being subjected to electro-aversive tortures and other therapies would have been able to just closet their desires to their clinicians in order to avoid the abuse. Reference: Marks, I., Gelder, M., Bancroft, J., & O’Neill, M. (1970). Sexual Deviants Two Years after Electric Aversion. British Journal of Psychiatry, 117(537), 173–185. doi:10.1192/S0007125000192864
Then in 1972 we have Richard Green, Lawrence Newman, and Robert Stoller (Green, R. (1972). Treatment of Boyhood “Transsexualism.” Archives of General Psychiatry, 26(3), 213. doi:10.1001/archpsyc.1972.01750210021003) practicing what they claim is a successful preventative treatment for “boys” from becoming full blown adult trans women as they get older. The abstract shows very clearly how their affinity for feminine habits and identity are considered problematic and in need of fixing by having a strong male role model to butch them up, pre-saging the more recent phenomenon in the “detransitioner” community of attempts to cure dysphoria in transmasculine people through consciousness raising sessions with lesbian women to reinscribe a supposedly proper female identity on the individual.
Based on retrospective reports of adult males who want to change sex, we have identified preadolescent boys at high risk for the development of adult transsexualism. These boys prefer the dress, toys, activities, and companionship of girls, and state their wish to be girls. During the past four years we have treated five very feminine boys and their parents. Treatment consists of developing a close relationship between a male therapist and the boy, stopping parental encouragement of feminine behavior, interrupting the excessively close relationship between mother and son, enhancing the role of father and son, and generally promoting the father’s role within the family. Results indicate the capacity for gender role preference in the preadolescent male to undergo considerable modification toward masculinity.
Despite claims of success, the “boys” in the Green, Newman and Stoller article were very young (as young as 5) at the point of treatment, and still very young years later at the point where treatment was considered to have been successful (some at 9 years old!). There’s rife misogyny throughout the text — they blame overbearing over-intelligent and sensitive mothers for having somehow created their children’s failures to bond with their male role model. Their accounts also have decidedly homophobic conversion therapy features to them:
The boy has made a considerable shift in his gender-role orientation. He no longer crossdresses, no longer improvises feminine costumes, and never takes the role of a female in games. When he draws pictures, they contain men, whereas previously they had always been of women. He plays well with boys and is accepted by them, no longer being an object for teasing. He fantasies himself, in the future, as a husband and father. Residual feminine identifications are evident in an occasional feminine gesture and an interest in long, silky men’s bathrobes and other clothing which can take on a flowing gown-like quality; however, he is decidedly masculine and comfortable in his new role.
The children in this piece appear to find ways to sublimate their feelings into models which are acceptable to the people who are in control of every aspect of their lives, and learn to perform heterosexuality as much as masculinity in how they go ahead.
We also have three extremely dubious pieces by a D.H. Barlow, starting in 1973 (Barlow, D. H. (1973). Gender Identity Change in a Transsexual. Archives of General Psychiatry, 28(4), 569. doi:10.1001/archpsyc.1973.01750340089014).
This claims in to be “the first successful change of gender identity in a diagnosed transsexual”. From the abstract:
After initial attempts to change patterns of sexual arousal and suppress central transsexual fantasies failed, components of female role behavior in a 17- year-old male transsexual were defined, measured, and modified piece by piece. Male and female components of sitting, standing, and walking were identified and changed from feminine to masculine. Next, masculine social behavior and vocal characteristics were instigated; following this, male sexual fantasies were initiated and strengthened. At this point attempts to change patterns of sexual arousal from homosexual to heterosexual, which had failed earlier, were successful. In many instances the procedures were experimentally demonstrated to be responsible for changes. These data indicate that gender role may not be as inflexible as assumed.
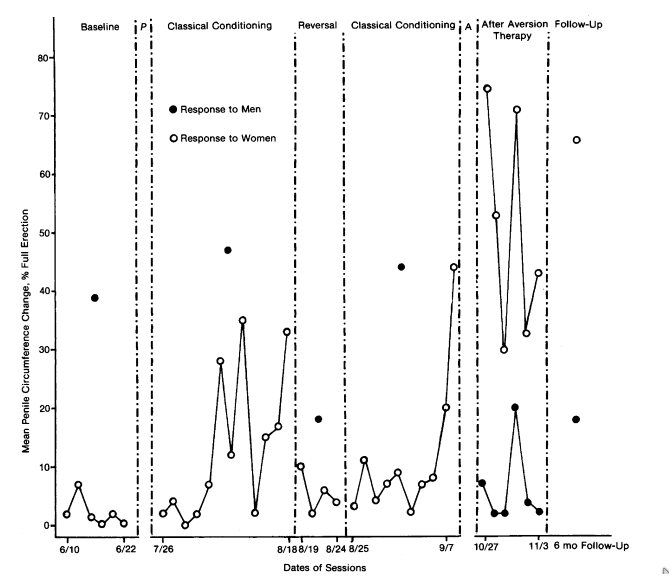
Again, the transphobic change effort is indistinguishable from homophobic conversion efforts. A range of behavioural training including electro-aversive shocks applied to the patient which would stop when the patient reported no longer experiencing the fantasy. In this study one of the numerous metrics undertaken to provide a gloss of objectivity was penile plethysmography (using a gauge to measure the circumference of the penis), while instructing the 17 year old trans girl to imagine a heterosexual fantasy for as long as she was able. The patient was required to signal when she had successfully achieved a clear mental image and then when a transsexual fantasy had impinged upon it. It is clear that as a measure this is the sort of thing that an individual who knew what was expected of them might end up playing along with in order to escape the degrading treatment undertaken. The follow up for this case study involved confirming that the patient had a “steady girl friend” a year later. In a chilling quote from the piece:
“He reported that it was “now easier” to look and act like a boy and that he was getting better at it. However, he still felt like a girl, fantasized himself as a girl (both sexually and socially), and reported that if he had a choice at this time he would change his sex. Throughout this phase patterns of sexual arousal, as measured by penile circumference change, were homosexual with no arousal to women”
Barlow followed this with another piece in 1977 on the “successful” exorcism of a trans person. (Barlow, D. H., Abel, G. G., & Blanchard, E. B. (1977). Gender identity change in a transsexual: An exorcism. Archives of Sexual Behavior, 6(5), 387–395. doi:10.1007/bf01541182) This is interesting in so much as it reveals that the technology for engaging in medicalised conversion efforts was far from fully separate from religious conversion efforts. Barlow bemoans:
“Although the prevention of transsexualism is the ideal, work in this area has been fraught with ethical problems, and data on the possibility of prevention, or even what to prevent, are not available.”
This piece uses Barlow’s previous work in 1973 claiming to have tortured the transness out of a trans minor as well as a single case study of an M-t-F-t-M detransitioner (Money, J., Wolff, G. Sex reassignment: Male to female to male. Arch Sex Behav 2, 245–250 (1973). https://doi.org/10.1007/BF01541760) and the author’s pre-existing conviction that prevention of transsexualism is the ideal in order to justify the idea that there is hope (somewhere) for a cure for transness. This despite that Barlow1973 clearly took coercion, and Money-Wolff1973 documents a case of spontaneous regret by a transitioned person and subsequent detransition (despite the impossibility of surgical reversal, and with the consequent difficulties of the detransitioned person needing to reconcile themselves with their transitioned body, never mind that it did not constitute evidence that externally generated forces could induce a change in identity!). In a later 1979 piece Barlow notes in follow up of 3 cases he had previously discussed:
It is somewhat unusual for transsexuals to agree to enter psychotherapeutic treatment as an alternative to surgery. For the first case in the series, an adolescent, surgery was not possible and psychotherapy was chosen as an alternative that might relieve some current suffering, with surgery possible at a later date. The last two patients cited an inability to pass successfully as a woman (by their own standards) as determining factors, although other factors entered in, such as type of relationship possible after surgery and “incompleteness” of the surgical transformation.
Concerningly, the use of penile plethysmography in previous efforts to demonstrate what the researchers would clearly consider to be a successful change in gender identity and sexuality (these things are only starting to become slightly disambiguated by 1979) are not seen as problematic for the supposed objectivity of evidence secured via plethysmography, even when that change was brought about by a two hour faith healing session:
The notion that psychosocial intervention for transsexualism can be effective is further strengthened by the recent case report of a conservatively diagnosed transsexual well on his way to surgery who was “exorcised” of his mistaken gender identity by a faith healer in a matter of two hours.” Objective measures similar to those used in this study revealed stability in these changes at a two-year follow-up.
In contrast with that we have a piece by Miriam Oles (Oles, M. N. (1977). The transsexual client: A discussion of transsexualism and issues in psychotherapy. American Journal of Orthopsychiatry, 47(1), 66–74. doi:10.1111/j.1939–0025.1977.tb03245.x). She stresses both from direct contact with trans patients as well as from the available literature, that there hasn’t really been any particularly convincing evidence about effecting changes to people’s gender identity. It’s worth remembering here that in the cases where successful changes have been reported, these are all in very small numbers, often in the form of spontaneous (rather than therapist led) detransition, or under literally violent coercion techniques, out of much larger patient cohorts who were quite happily transitioning. Even the conversion therapists appear from their own writing to see these individual cases of transition reversal as major breakthroughs (amidst a patient base that mainly is trans and stays trans). Oles says (rather more conservatively):
Choice of Treatment
Those who have had contact with pre-operative transsexuals over an extended time are impressed by the degree of distress they experience and by the persistence of that feeling. The goal of treatment of gender dysphoric individuals, as with other clients, is to relieve their distress to whatever degree possible and to help them feel comfortable with themselves…
There are two possible treatment approaches for this condition. One is to change the identity to conform to the body; the other is to change the body to conform to the identity. A variety of psychological treatments have been used in efforts to achieve the former goal. These treatments have included classical psychoanalysis, behaviour therapy, and hypnotherapy. There has been very little success reported in treating adult transsexuals with these methods…. There have been recent reports of success in the behavior modification treatment of young boys whose behavior is considered to be “effeminate”. The long term effects of this treatment are not yet known, and it is highly controversial.Role of Psychotherapy
As research studies indicate, psychotherapy has not been successful in reconciling the gender identity of the transsexual with anatomy…
A figure who rises to significance in the 1970s is Lothstein, who is still cited as an inspiration by modern practicing psychotherapists attempting to carry out non-medical, non-transitioning psychotherapeutic treatment of Gender Dysphoria (many people would recognise this as a thinly disguised euphemism for using talking therapies in order to change someone’s gender identity — conversion therapy by any other name), such as Dr Az Hakeem who has recently gained some acclaim within the “Gender Critical” movement as a former television psychiatrist who will validate their beliefs that trans people can and should be deterred from transition for one reason or another.
“Our Clinic’s focus on psychotherapy as the treatment of choice represents a significant departure from other gender identity clinics throughout the country. We employ psychotherapy in an attempt to help stabilize the patient to adjust to a non-surgical solution to his problems. Our experiment has met with various degrees of success and failure.” — Lothstein, L. M. (1977). Countertransference reactions to gender dysphoric patients: Implications for psychotherapy. Psychotherapy: Theory, Research & Practice, 14(1), 21–31. doi:10.1037/h0087488. https://sci-hub.se/10.1037/h0087488
Lothstein’s idea here was that the reason that psychotherapy had so consistently failed in the past was that psychotherapists were failing to establish a “therapeutic alliance” with patients via dealing with issues around “countertransference” — a phenomenon whereby an emotional response is triggered in the therapist by the patient. Lothstein describes the majority of gender dysphoric patients as suffering from “severe narcissistic character disorders accompanied by a number of significant ego defects including a potential for regression and psychotic decompensation.” Psychotic decompensation is a general degeneration of mental state into psychosis (such as delusions and hallucinations). Although it’s relatively well known that trans people may be at a higher risk of mental health comorbidities (notably depression!), especially with untreated dysphoria, this doesn’t really seem to match a lot of the other prior literature on what transsexual people are like, and it isn’t clear whether this claim about psychosis is a particularly pathologising way of referring to ordinary phenomena of trans people experiencing ourselves the way we experience ourselves, or if Lothstein’s clinic happened to be full of particularly troubled patients. There is a plethora of further labels Lothstein throws out typifying transsexual patients by throwing the book at them:
A large number of patients who initially request SRS often leave the GDP program and are not available for study. The patients who remain in individual or group treatment present a constellation of traits which often includes a stable personality organization, a tendency to employ primitive defenses, a constellation of schizoid, obsessional traits, and the potential to decompensate under stress in a psychotic manner.…
Psychological and psychiatric diagnoses of our patient group confirms the prevalent diagnostic category of patients requesting SRS to be either Borderline Personality Organization or Latent Schizophrenia. As a group, patients diagnosed as having a Borderline Personality Organization or Latent Schizophrenia are rarely seen in intensive psychotherapy as they tend to be exceedingly difficult cases to treat and often need hospitalization to control their impulsivity and destructive acting out.
In a field of classification for mental illness, it seems like for Lothstein, transsexual people have the whole package, narcissistic, delusional, schizophrenic, manipulative, controlling and “blocking”, i.e. resisting the efforts of the psychotherapist to urge the patient to cease their desire to medically transition. It’s clear that being a patient of a therapist like Lothstein, who was very clearly not interested in assisting with transition, will have been an absolutely awful experience for trans people in his care. In fact the Digital Transgender Archives contain many pieces where trans people express their disgust for Lothstein’s reparative approaches, such as a review of his book on FTM transsexuals in this magazine by a trans man in 1984:
I find it, notwithstanding, to exude a cold clinical approach, which is at once dehumanizing and devoid of compassion, not to mention insensitive and insulting. For example, the author uses female pronouns exclusively — even when referring to post-operative F-M TSs who are now — by definition, and for all practical purposes — men. …
In summary, I propose that Lothstein ‘s book is as potentially damaging to the TS “cause” as Janice Raymond’s THE TRANSSEXUAL EMPIRE: The Making Of A She-Male. Both books contain primary assumptions that are unwarranted and invalid. …
Lothstein’s approach to the problem is theoretical, clinical and psychoanalytical — in specific, (neo-) Freudian. Raymond’s approach to the phenomenon is ideological, sociological and sexo-political — in particular, radically feminist. The transsexual’s perspective, on the other hand, is experiential, existential and phenomenological — ie. a unique, personal sense of one’s self-identity (including one’s body-image).
—Rupert Raj, B.A. editor of Metamorphosis Newsletter.
Here we have a report from an exorcism of a trans person — Barlow, D.H., Abel, G.G. & Blanchard, E.B. Gender identity change in a transsexual: An exorcism. Arch Sex Behav 6, 387–395 (1977). https://doi.org/10.1007/BF01541182
“Patients who believe themselves to be transsexuals represent a unique challenge to the therapist. Perhaps they, more than any other group, present themselves with both an established diagnosis and a predetermined decision as to their management. They are not the typical client seeking a diagnosis and therapy from the therapist. They are seeking from the therapist the final validation of their own diagnosis, which will then permit a sex-change procedure, performed by a surgeon, which they have already deemed essential to their cure. The therapeutic challenge and duty is to question the diagnosis. Is the proclaimed transsexual truly transsexual?”
— Shtasel, T. F. (1979). Behavioral treatment of transsexualism: A case report. Journal of Sex & Marital Therapy, 5(4), 362–367. doi:10.1080/00926237908407080 — https://sci-hub.se/10.1080/00926237908407080
1980s
“None of the patients in our sample was first recognized as having a severe gender disorder by their primary care physician ; initial recognition usually came from authorities, friends’ parents , specialist physicians , or law enforcement agencies . In some cases the patient’ s primary pediatrician or family physician had responded to the parents’ fears by telling them their child would outgrow the disorder . None of the patients , however, outgrew their gender identity conflicts; 21 patients , however , wished that their problems would go away.”
— Lothstein, L. M. (1980). The Adolescent Gender Dysphoric Patient: An Approach to Treatment and Management. Journal of Pediatric Psychology, 5(1), 93–109. doi:10.1093/jpepsy/5.1.93
“The dictum that transsexualism is resistant to psychotherapy has led many investigators to view sex reassignment surgery (SRS) as the treatment of choice and dismiss psychotherapy as unfeasible. The Gender Identity Clinic at Case Western Reserve University, Cleveland, was organized to treat transsexuals with individual and group psychotherapy and SRS. Of 50 gender dysphoric (GD) patients, 70% have adjusted to nonsurgical solutions, 20% are receiving treatment, and 10% have received SRS and psychotherapy. The crux of psychotherapy is establishing a therapeutic alliance; this is aided by the context of the Gender Identity Clinic. Clinical evidence suggests that new therapeutic techniques may enable psychotherapy to become the treatment of choice with most GD patients and that psychotherapy and SRS are not mutually exclusive. Most patients request and benefit from psychotherapy after SRS. (Arch Gen Psychiatry 1981;38:924–929)”
— Lothstein, L. M. (1981). Expressive Psychotherapy With Gender Dysphoric Patients. Archives of General Psychiatry, 38(8), 924. Notably looks like one of the first instances of the modern variety of transgender conversion psychotherapy. doi:10.1001/archpsyc.1981.01780330082009. https://sci-hub.se/10.1001/archpsyc.1981.01780330082009
1990s
Joe Nicolosi, Paul McHugh, the rise of NARTH and Zucker. [fill me]
2000s to present day
By this point, the consensus against attempts to cure people of gender dysphoria had finally started to solidify for the most part. There remained however outliers, both in the UK and in North America. In the UK there was Dr. Az Hakeem, who insisted on a psychopathological understanding of trans people’s identities.
“If the definition of a delusion is that of being a firmly held, unshakeable false-belief then surely the conviction that one is what one is not is also understood as a delusional disorder.” — Dr. Az Hakeem, Trans-Sexuality: The Emperor’s New Clothes (2007)
Finally we get to conversion therapy in present day trans healthcare. A significant figure for UK at least, is Dr Az Hakeem. Hakeem documented his practices running a “no medicine” clinic for a while under the NHS, (Hakeem, A. (2012). Psychotherapy for gender identity disorders. Advances in Psychiatric Treatment, 18(1), 17–24. doi:10.1192/apt.bp.111.009431).
In the paper he makes clear he bases his approach entirely on Lothstein’s research:
“The literature on group psychotherapy for gender identity disorders yields only nine papers: Lothstein and his colleagues at the Case Western Reserve University Gender Identity Program in Ohio have described their work with expressive group therapy (Lothstein 1977a,b, 1979, 1981; Althof 1980) and in more recent years I have published in this area (Hakeem 2007, 2008, 2010a,b).”
As we described earlier, Lothstein’s practice was entirely oriented around psychotherapeutic attempts to cure trans people of our gender identity “disorder”, and it should be no surprise that a policy at Az Hakeem’s clinic specifically did not refer people for endocrine and surgical treatment. His work has also been adopted largely by Sheila Jeffreys and the “Gender Critical Therapist” movement who have been making loud noises against a conversion therapy ban potentially impacting their ability to practice… What exactly? Indeed.
